SCC oesophagus with leiomyomata of stomach


Barium meal showed a tight stricture at the lower third with food debris above it.
It was reported as "probably a benign stricture with no irregularity and no shouldering". No further films were taken to outline the stomach or gastric outlet.
At endoscopy the stricture was dilated enough to allow biopsy. The biopsies demonstrated squamous carcinoma of the oesophagus.
CT scan showed some thickening in the lower third of the oesophagus but it was difficult to demonstrate any actual tumour. In addition it showed a "mass indenting the lesser curve of the stomach, probably coeliac nodes". "This is probably not a curable tumour"
.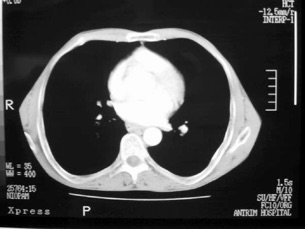


Incidentally the tumour was also apparent on the plain chest Xray film as a space occupying lesion within the stomach impinging on the gastric air bubble.
The patient was referred to the regional oesophageal service for further management.
Review of the CT films suggested that the gastric tumour was actually a benign leiomyoma (stromal tumour) of probable long-standing. The oesophageal tumour itself was relatively early. (Endoscopic ultrasound was not available.) Repeat endoscopy with examination of the stomach confirmed that the oesophageal tumour was very small and that there were two smooth, rounded, submucosal tumours, one at the cardia and the other on the lesser curve in the antrum (photos not available). Endoscopy also confirmed the CT appearance which suggested that a gastric tube could still be fashioned and used as a conduit to replace the oesophagus.
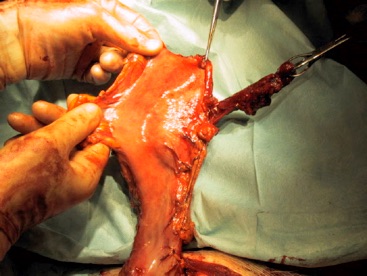
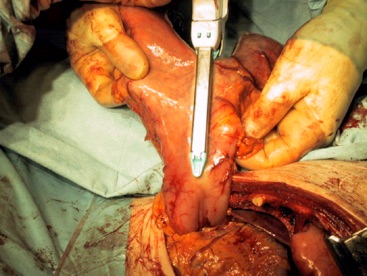
Using a TCT 75 stapler (Ethicon) it was possible to fas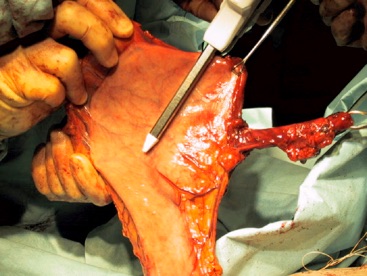 hion a long gastric tube, excising the cardia with its leiomyoma and the second leiomyoma more distally.
hion a long gastric tube, excising the cardia with its leiomyoma and the second leiomyoma more distally.
The patient was extubated in the recovery ward and transferred to the high dependency unit with epidual, minitracheostomy, apical and basal chest drains but no nasogastric tube. His recovery was uncomplicated and he left hospital on the 7th postoperative day.
Pathology revealed a T1 (mucosal invasion only), N0 tumour with good prognosis. The stromal tumours showed no sign of malignancy, with low mitotic rate. However, the prognosis from such tumours is difficult to predict on histological grounds alone.
