Decortication for Empyema

62 year old man had been treated by his GP for cough associated with shortness of breath and chest tightness for 14 weeks before referrral to a general physician. He had never smoked or drunk alcohol, had no history asthma, exposure to respiratory pathogens or foreign travel. He had however, lived close to a shipyard and could not rule out asbestos exposure. He was treated for a number of weeks for "chest infection" before referral to a respiratory physician.

At this stage there was general malaise, loss of stamina and night sweats and a "tightness" in the chest. The chest Xray (right) showed:
•loss of volume in the left hemithorax
•pleural effusion
•air fluid level
•consolidated lung
•raised left hemidiaphragm
•crowding of the ribs of the left hemithorax compared to the right

The CT scan confirmed these findings with most of the opacity having an attenuation value higher than free fluid but not that of solid tissue.The volume of the left thoracic cavity was seen to be reduced. In addition there was a thick rind trapping the lung and coating the parietal pleural surface.
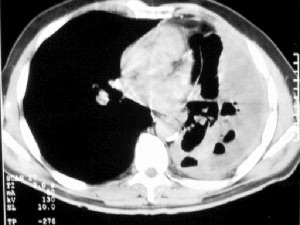
In the lower images there were pockets of air associated with previous attempts to aspirate fluid for diagnosis.
Surgical referral "for thoracoscopic pleural biopsy".
On review of the history there was very little pain. The main symptoms was loss of stamina, malaise, night sweats and breathlessness on exertion. The examination revealed loss of volume and movement on the left side, with associated dullness to percussion.
Working diagnosis: Empyema
Differential diagnosis: Mesothelioma
Rather than a thoracoscopic biopsy, I opted for decortication and parietal pleurectomy because:
•there had actually been minimal asbestos exposure
•there was little pain
•a small pleural biopsy may not be diagnostic for mesothelioma whereas a complete pleurectomy specimen would leave no doubt
•even if mesothelioma was the diagnosis decortication/pleurectomy would provide good palliation of breathlessness and
•debulking of any disease
•if empyema it was likely to be at fibrotic stage which would leave long term debility
Surgery

Findings: Half inch thick pleura with foul smelling pus (sent for culture and grew bacteroides)
Procedure: Decortication of the left lung with parietal pleurectomy.
In the recovery ward the lung was seen to be well inflated on chest Xray. There was minimal air leak.
Postoperative progress
Over the next few days the chest Xray deteriorated but the lung remained inflated.
Such a course is common post decortication. Pneumonitis develops in the areas which had been previously consolidated and trapped. It needs no specific treatment.

Once the drains had been removed and the patient was moving freely there was clearing of the post-consolidation pneumonitis though there was residual tenting of the diaphragm laterally.

After 3 weeks there had been marked resolution of the pneumonitis with further expansion of the lung.
At 8 weeks the patient was back to walking his dog a number of miles per day. He commented that his heart rate which had been sitting around 90/min in the weeks before the surgery had returned to his normal of 60/min. There remained some numbness anterior and above the wound but this was controlled with occasional paracetamol (acetaminophen). The night sweats had abated and he was considering returning to work.

The chest Xray showed further improvement with resolution of some of the lateral pleurally-based shadowing.
Final Diagnosis:
•Empyema thoracis
•Bacteroides on culture suggests possible aspiration - no underlying cause identified though gastroscopy pending.
