Paralysis of the diaphragm following blunt trauma

A 67 year old delivery driver’s van was struck from behind. He was knocked unconscious and injured his left lower lateral ribs as the “seatbelt went up and underneath my ribs”. After initial assessment he was discharged from a district hospital. However, he remained unwell and re-presented to hospital two weeks later with weakness and a near collapse. On admission he had left sided chest pain, his oxygen saturation was 95% on room air and examination by the casualty officer revealed decreased air entry at the left base.
Investigations:
Chest x-ray showed elevation of the left hemi-diaphragm consistent with ruptured diaphragm.

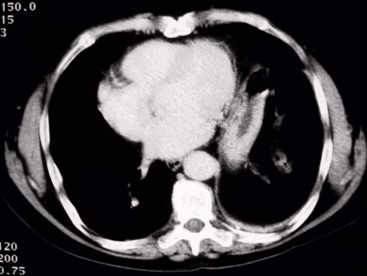
CT scan of chest was reported as also being consistent with a rupture of the diaphragm.
Surgery:
On exploring the left thoracic cavity there was no evidence of a rupture of the diaphragm though the diaphragm itself was significantly raised consistent with paralysis. There was significant atelectasis of the left lower lobe. The left hemi-diaphragm was plicated. The aim of the operation is to tighten the paralysed diaphragm with plicating sutures. This improves the efficiency of ventilation by the chest wall muscles and the contra-lateral hemi-diaphragm.
Progress:
Following the surgery the patient made good progress and was discharged on postop day 5. He was able to return to work part-time after 8 weeks. However, he is only able to lift small boxes compared to the sides of beef he used to lift. At 12 months following the injury he reports some left thoracotomy wound pain, shortness of breath on walking up a hill and easy fatiguability. Examination reveals tenderness of the left costal margin at the level of the 8th rib in the anterior axillary line and reduced chest wall movement at the left base.
The postoperative X-ray showed bilateral atelectasis but an improvement the left hemi-diaphragm.

The late followup chest X-ray shows persistent elevation of the diaphragm but an improvement on the post-injury status.

Comment:
This man suffered a significant chest injury which was under estimated at the time of his initial consultation. The mode of injury would seem to be, as the patient himself suggested, that the sash portion of the lap sash seatbelt has impacted on the left costal margin forcing it against the underlying lung, the underlying diaphragm and probably of more relevance the phrenic nerve. The phrenic nerve runs down over the pericardium and enters the diaphragm just deep to the area of tenderness in the left costal margin.
The phrenic nerve can also be injured in association with a cervical injury - either fracture or torsion.
When a hemi-diaphragm is paralysed it moves paradoxically with each breath. Instead of contracting and descending towards the abdomen increasing the volume of the lung it is actually drawn up into the chest reducing the volume of the lung during respiration. Therefore there is an exaggeration of the lung collapse and the respiratory embarrassment when a paralysed diaphragm is present. The operation of plication of the hemi-diaphragm tightens the diaphragm like a drum so that it does not move at all during respiration. This allows the contra-lateral diaphragm and chest wall muscles to work more efficiently. It does however leave a significant degree of respiratory handicap. This would be consistent with the symptoms of breathlessness on exertion or walking up hills.
This injury is probably missed more often than we realise. The appearances may be mimicked by atelectasis and volume loss due to pain and sputum retention. However, there should still be movement of the diaphragm on fluoroscopy. Phrenic nerve injury can also occur due to injury in the neck, usually a penetrating or iatrogenic injury.
The natural history is not clear. Some phrenic nerve palsies recover spontaneously but this may take over 12 months. Plication of the diaphragm may allow weaning from a ventilator, or, as in this case, a quick discharge from hospital and return to light manual work. One may surmise that in the long run, if a spontaneous recovery were to occur, the plication would decrease the function of the diaphragm.
