Rubber Bullet Injuries

During the recent civil “Troubles” in Northern Ireland, the security forces frequently have found themselves between rioting groups of youths from different factions. The problem of “reasonable force” has led to the development of “rubber bullets”, officially called baton rounds. These are not rubber and bear little resemblance to a bullet. Made of hard plastic, these cylinders are approximately 15cm long and 4cm in diameter. When used according to the official directions, fired at the ground in front of the rioter, they would be expected to cause little pathology. However, a direct hit to the head or the chest....

During a confrontation at a sectarian “interface”, a youth collapsed after receiving a blow to the chest.
The bruise on his chest wall suggested a relatively minor injury.
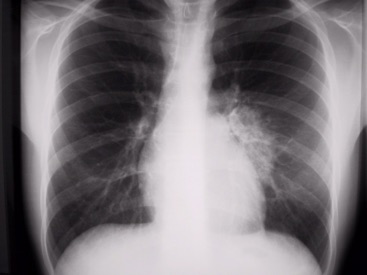
The initial chest X-ray was virtually normal. However, the close-up does show some shadowing adjacent to the pericardium.
However, the man's symptoms of pain and breathlessness suggested something more severe. Because of hypoxaemia on blood gas analysis (p02 8.60kPa, pCO2 6.20kPa on room air), the patient was admitted.
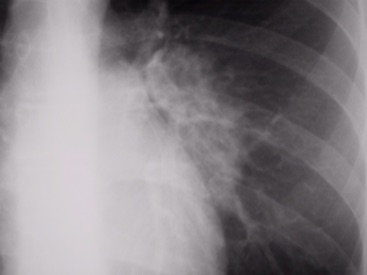
The repeat chest X-ray shows why the symptoms were out of proportion to the minor skin wound. There is now more extensive contusion in the left lower lobe. The initial X-ray actually showed some loss of the left heart border. By the time the second x-ray has been taken, the intra-alveolar bleeding has extended throughout the lingula and the upper lobe. The preservation of the silhouette of the diaphragm suggests that the lower lobe has been spared. Of note, the radiological picture lags the clinical picture by about 24 hours, the patient improving by the time this X-ray was taken.
There is now more extensive contusion in the left lower lobe. The initial X-ray actually showed some loss of the left heart border. By the time the second x-ray has been taken, the intra-alveolar bleeding has extended throughout the lingula and the upper lobe. The preservation of the silhouette of the diaphragm suggests that the lower lobe has been spared. Of note, the radiological picture lags the clinical picture by about 24 hours, the patient improving by the time this X-ray was taken.
Frequently lung contusion which results in loss of alveoli is accompanied by relative pulmonary arterial diversion. Therefore no shunt occurs so blood gas analysis is almost normal.

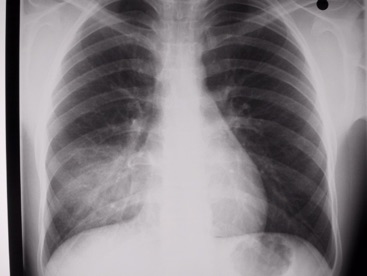
His right sided injury was apparent on the initial X-ray which was taken only because his injury was similar to that of his cousin who had been admitted earlier in the evening.
Both patients recovered in a matter of days without consequence. The treatment, as with all chest trauma, was oxygenation, pain relief and respiratory physiotherapy. A repeat X-ray at 4-6 hours is indicated in all chest injuries. In this case it is more for the diagnosis of late pleural effusion or pneumothorax rather than to follow the course of the contusion.
