Late imaging of ruptured diaphragm

56 year old man presented with a "chest infection".
A chest Xray was requested by his GP because he had been a long-term smoker. The chest Xray showed an elevated right hemidiaphragm adjacent to some healed rib fractures.
Further questioning revealed that he had been involved in a road traffic accident 7 years previously. He had suffered:
•4 fractured ribs on the right
•a pelvic fracture
•a fractured right clavicle
•a "punctured lung"
He had made an uneventful recovery after chest drain insertion. His only ongoing symptom was a "niggling" pain in the right lower ribs.
Imaging
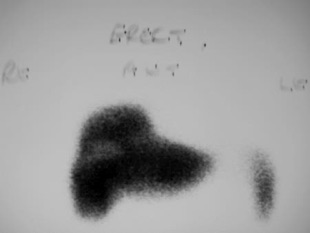
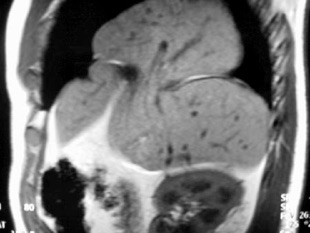
Liver scan showed a "bilobed" shape which when compared to the MRI scan images demonstrates clearly the liver herniating through the defect in the dome of the diaphragm.


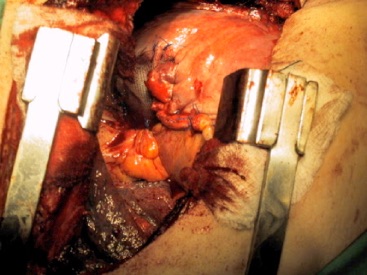
Surgery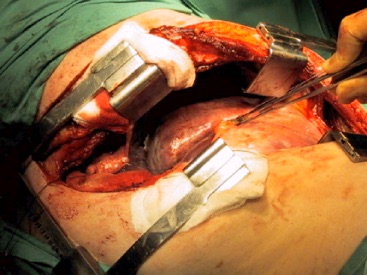
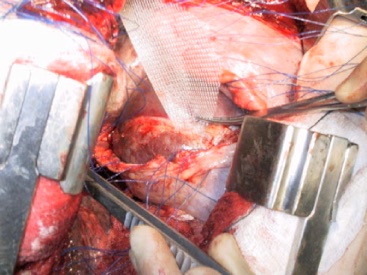
A right thoracotomy was performed because it was felt that there would be adhesion formation to the herniated liver. However on exploration there were virtually no adhesions. A portion of the liver was seen to have herniated through a tear in the dome of the right hemidiaphragm. (the forceps mark the free edge of the torn diaphragm. The herniated liver is seen in the middle of the picture). The diaphragmatic defect was extended medially and laterally to allow reduction of the herniated liver.
Lessons
There is no "late rupture" of the diaphragm, only late diagnosis.
Ruptured diaphragm should be considered when there has been:
•compressive trauma to the abdomen
•fractured pelvis
•fractures to the lower ribs
Artificial ventilation may keep the abdominal viscera reduced and the injury may not be evident on early chest films. As spontaneous breathing resumes there is a relentless vacuum pulling the viscera into the chest. By this time the patient is probably at home or on a fracture ward and diagnostic chest Xrays have ceased to be a priority!
In general an acute diaphragmatic rupture should be approached via laparotomy as there are likely to be associated abdominal injuries. When the diagnosis has been delayed it is usually thought wisest to approach from a thoracotomy as there may be extensive adhesions to the lung, pleura and rib fracture sites.
