Chest Drainage Systems


Chest drains hold a degree of mystique for many doctors and nurses. The introduction of newer drainage systems has been of major assistance to those familiar with their indications and usage. However, it has added to the confusion for those less familiar with chest drainage. This is a guide to assist in the use of commonly available drainage systems.
Chest drains are used to treat pneumothorax, haemothorax, empyema and other collections within the pleural cavities. The introduction of underwater seal drainage in the 1870’s was a major advance in the treatment of thoracic diseases in that it allowed surgeons to safely open the pleura knowing they would be able to re-expand the lung at the end of the procedure.
A chest drain system involves four components:
•drain tubing
•a valve (underwater seal or flutter valve)
•a collection chamber
•suction control device (optional)
There are now a number of drainage systems available. Portability has been a major factor driving development as early mobilisation and gentle exercise are important factors in pulmonary rehabilitation.
Types of Drainage Systems
Underwater Seal Bottles
The classic underwater seal drainage system requires three bottles connected by tubing.
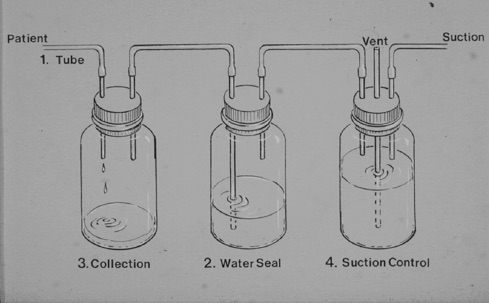
The first bottle provides the collection chamber. The second, the water seal valve, has an afferent tube which is kept below water level. Fluid and air can egress from the tube. The vacuum produced by inhalation draws fluid into the tubing but does not allow air to be re-introduced to the pleural cavity. The intrapleural vacuum can be countered by the application of suction to the third bottle, the suction control. In addition to the afferent and efferent tubes the suction control bottle has a third tube open to air. The depth the tube penetrates below the fluid level determines the degree of suction. Hence the familiar measure of surgical suction, centimetres of water.
The major disadvantage of the three bottle system is that it is cumbersome and not particularly portable. The bottles must be kept upright to maintain the water seal valve. Breakage of the glass bottles is a potential problem.
Three chamber plastic compartmentalised drainage systems (e.g. Pleurovac)
Using non breakable plastic the three bottle system can be incorporated into a single unit (Figure 2). This compact drainage system allows greater convenience and portability. It can be used with standard surgical suction, the vacuum being controlled by the height of the column of water in the vacuum control chamber. Some systems also measure the vacuum being produced by the patients respiration. 
However, the bottles are still bulky and must be maintained upright to maintain the water seal. Of necessity the patient must remain in hospital where proper nursing supervision is available. The tubes should not be clamped lest a tension pneumothorax develop, the fluid in the water seal chamber must be maintained above the level of the afferent straw at all times and, to prevent siphoning of fluid into the chest, the bottles must be kept below the level of the patient.
How to connect a three chamber system system
•Pour water into water seal chamber to level indicated on bottle.
•Pour water into suction control chamber to the required level (usually 15-25 cm water). (When the 20cm is divided into 2 x 10cm chambers as in the Redax drains, the tap on the rear of the chamber should be set to ‘open’, the chambers filled to the marked level, shaking the bottle to allow water to fill both chambers equally, then the tap on the rear set to ‘off’ and the cap replaced on the chamber.)
•Connect the chest drainage tubing to the collection chamber.
•Connect the suction tubing to the vacuum source.
Dry suction, Dry Valve Chest drains
The simplest systems to set up are those with a dry valve and a dry suction control. 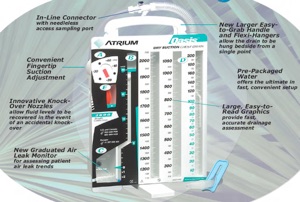 The advantage of these is that all that needs to be done is connect the tubing to the drain. Also, if they fall over, the valve systems are not compromised by fluid flowing into other chambers. Unfortunately some manufacturers have added the ‘feature’ of an air leak indicator (designed to grade the amount of air leak). This has to be filled with fluid so the setup is not as simple as one would like. These systems also tend to be more expensive than the wet drains.
The advantage of these is that all that needs to be done is connect the tubing to the drain. Also, if they fall over, the valve systems are not compromised by fluid flowing into other chambers. Unfortunately some manufacturers have added the ‘feature’ of an air leak indicator (designed to grade the amount of air leak). This has to be filled with fluid so the setup is not as simple as one would like. These systems also tend to be more expensive than the wet drains.
Plastic chest drainage bottles without suction control
The advent of reliable high volume, low pressure suction devices has allowed the development of simpler and less expensive drainage bottles. Consisting of an underwater seal chamber and a drainage, these bottles are lightweight but robust and are simpler to set up than the three chamber system . The vent port connects to a thoracic suction device 2kPa high flow, low pressure) to regulate suction.
How to connect a plastic bottle system
•Pour water into water seal chamber to a depth of 3 cm (level indicated on bottle).
•Screw the chest drainage tubing with its incorporated straw into the water seal chamber ensuring a tight seal without cross threading.
•Connect the vent port to the suction device tubing (the pressure in kilopascals approximates to a tenth of the pressure in centimetres of water).
•A cough will produce movement in the column of water in the straw though suction may dampen the swing. Bubbling indicates a persistent air leak.
Isolating and disposing of drainage bottle
-
•Tubing should be spigotted (or a secure knot tied).
-
•The bottle should then be double-bagged and disposed of with other contaminated waste.
Heimlich valve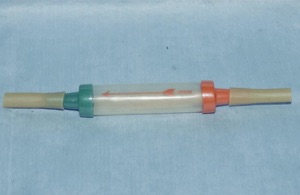
The Heimlich device consists of a rubber flutter one-way valve within a rigid plastic tube which connects to standard chest drain. It does not need to be kept upright like the underwater sealed drain and therefore is suitable for outpatient use. However, the efferent portal of the Heimlich valve must be kept open to the atmosphere making control of the fluid effluent difficult. The device is bulky under clothing and staining is a constant problem.
Ambulatory Chest Drainage System (Simms/Portex) - "Portex bags" [no longer available]
A development of the Heimlich valve principl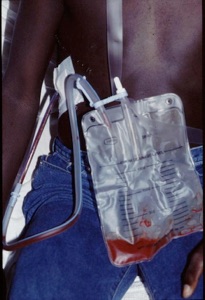 e was the Portex ambulatory chest drainage system. Unfortunately it is no longer available but alternatives exist. These systems are portable, do not need to be kept upright and provides hygienic drainage of the drain effluent. They consist of a dry valve (often a flutter valve) within a drainage bag or rigid box. Originally designed for battlefield use, the Portex bags were tested successfully following thoracic surgery in both an inpatient and outpatient setting (1). The bag was flexible, worked in any position and could easily be worn under clothing. The principle of the portable drainage system has been proven providing a convenient, hygienic solution which allowed early mobilisation and discharge from hospital.
e was the Portex ambulatory chest drainage system. Unfortunately it is no longer available but alternatives exist. These systems are portable, do not need to be kept upright and provides hygienic drainage of the drain effluent. They consist of a dry valve (often a flutter valve) within a drainage bag or rigid box. Originally designed for battlefield use, the Portex bags were tested successfully following thoracic surgery in both an inpatient and outpatient setting (1). The bag was flexible, worked in any position and could easily be worn under clothing. The principle of the portable drainage system has been proven providing a convenient, hygienic solution which allowed early mobilisation and discharge from hospital.
One disadvantage of the Portex bag was the inability to connect to suction. Therefore the lung needed to be adequately expanded off suction prior to connection to the ambulatory bag.
The Atrium Express Mini 500 rigid plastic system overcomes this disadvantage but has a relatively small collection chamber. This can be aspirated with a syringe. The Rocket flutter valve bag also has a small chamber and over-filling can clog the charcoal filter. New designs are promised. Disconnection, kinking of the tubing or obstruction by lying on the bag are potential dangers. Education of the patient or carer is important to avoid such complications.
Suction
One of the main differences in the available drainage systems is the method used to manage suction:
•A patient who is free from pain, to the degree that an effective cough can be produced, will generate a much higher pressure than can safely be produced with suction.
•If a patient cannot re-inflate his own lung, high volume, low pressure "thoracic" suction in the range of 15 - 25 cm of water can help.
•Patients on mechanical ventilators cannot produce an effective cough and therefore suction is advised.
•Suction which is not working properly is the equivalent of a clamped drain.
Close surveillance is therefore required by nursing staff trained to recognise faults in the drainage and suction system. It is better to remove suction than to use a faulty device.
References
1.Randomised clinical trial of chest drainage systems. Graham ANJ, Cosgrove AP, Gibbons JRP, McGuigan JA. Thorax 1992;42:461-2
