
A 46 year old otherwise fit man presented with increasing shortness of breath on exertion. An erect chest Xray showed what seemed to be a 'raised hemi-diaphragm'.
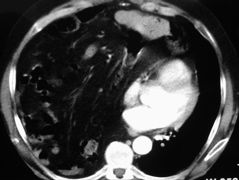
A CT scan demonstrated that the shadowing was due the presence of viscera in the chest, due to a diaphragmatic hernia either congenital or traumatic. The cardiac shadow and other mediastinal structures can be seen displaced by omentum and bowel in the right pleural cavity.
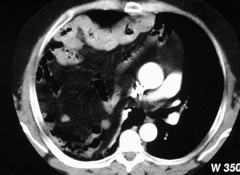
Colon can be seen clearly with omentum and small bowel high above the hilum of the right lung.
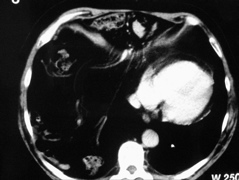
Strands of omentum can be seen sweeping over the free edge of the diaphragm, through an anterior midline hernial orifice. This represents a congenital hernia of the foramen of Morgagni. Colon and other bowel can be seen in cross-section. The heart is displaced back and to the left.

The topogram taken at the time of CT is with the patient supine. The full extent of the hernia is apparent. This is consistent with the patient's reported dyspnoea on lyng flat.

Three ports sufficed for the laparoscopic repair. The 10mm camera was inserted via a sub-umbilical cut-down with two 10mm ports in the right and left hypochondrium to allow grasping instruments to reduce the hernia contents and pass sutures.

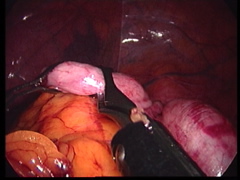
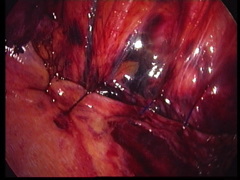
On laparoscopic exploration of the abdomen, the defect can be seen with bowel and omentum herniating into the chest.
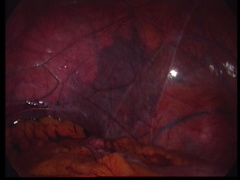
Atelectatic lung can be seen in the distance, separated from the hernia by pleura.
Bowel and omentum were retrieved using a 'hand-over-hand' movement with two endoscopic Babcock forceps.
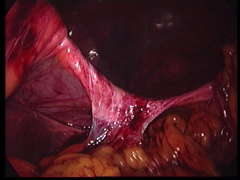
Omental and peritoneal adhesions remained adherent to the free edge of the diaphragmatic hernia.
Adhesions between the hernial sac and the diaphragmatic edge were divided with the endoscopic Ligasure device.
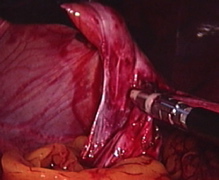
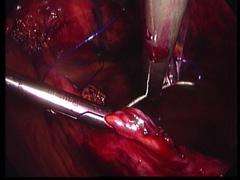
As no muscular diaphragmatic remnant exists anteriorly into which one can reliably place a suture or fix a patch, the plan was to suture the edge of the diaphragm to definitive anterior abdominal wall structures, burying the knots in small cutaneous incisions along the costal margin. Interrupted 2/0 Prolene sutures on a straightened needle were passed through the anterior abdominal wall. The terminal branches of the internal mammary vessels can be seen in the right limit of the hernia. The xiphisternum is seen projecting into the middle of the defect to the right side of this photo. The left mammary vessels passed through the contralateral limit of the defect confirming that a Morgagni hernia is indeed a midline hernia.
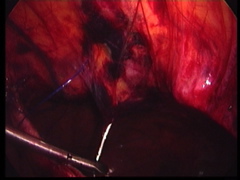
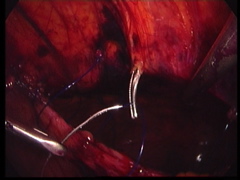
The needle was then passed through the free edge of the diaphragm.
The sutures were then retrieved through the abdominal wall. Each suture was placed either around the costal margin or over a broad bundle of rectus abdominis muscle. To ensure appropriate placement of the suture, a mosquito forceps was placed through the abdominal wall from the external cutaneous incisions. The suture was grasped adjacent to the needle and drawn through the wall.
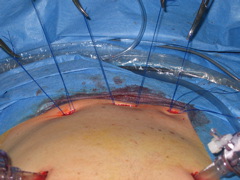
Eight sutures were placed through the anterior abdominal wall, through the free edge of the diaphragm and back through the abdominal wall. The three cutaneous incisions allowed the knots to be buried.
The sutures were tighten and tied in turn closing the defect without tension.
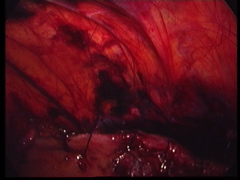
A final endoscopic view of the completed repair.

The postoperative chest X-ray shows re-expansion of the right lung. The horizontal fissure is depressed either due to persistent postoperative atelectasis or congenital hypoplasia of the right lower lobe.