
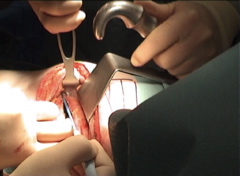
The patient is placed in a lateral decubitus position. The arm may be placed in a arm rest, though allowing it to fall forward over good padding will open up the auscultatory triangle. The epidural cannula can be seen in situ.

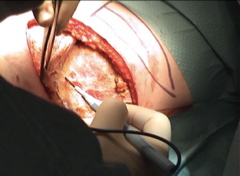
The patient is prepped and draped in routine fashion. The skin incision and its relation to the scapula are marked in ink.
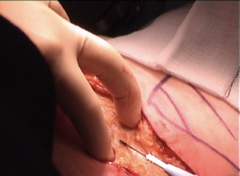
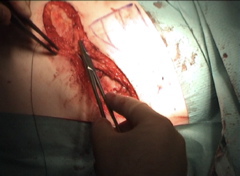
The skin is incised with a scalpel; fat and fascia are divided with cautery as far as the muscle fascia.
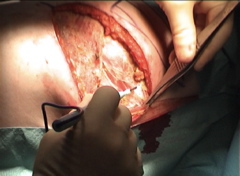
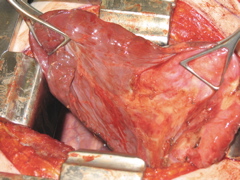
Subcutaneous flaps are developed. The outline of the auscultatory triangle can now be seen with the latissimus dorsi anteriorly, trapezius posteriorly and the scapula superiorly.
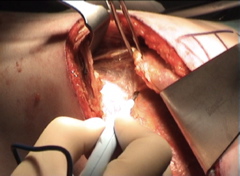
An incision is made in the fascia along the anterior border of trapezius posteriorly and the posterior border of the latissimus dorsi.
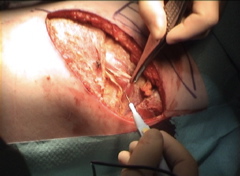
The triangle of fascia between the trapezius and latissimus is raised, exposing serratus and the rhomboid muscles deeply. The fascia can be excised but I generally keep it and use it to re-align the muscles when closing.
The latissimus is freed from the underlying serratus. Much of this dissection can be performed bluntly. However, care must be taken not to damage the neurovascular supply to serratus, which lies on the superficial surface of the muscle.
Similarly, trapezius is freed from the underlying rhomboids.
The serratus fascia is now incised as in a standard postero-lateral thoracotomy.
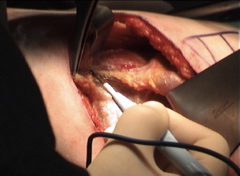
Carrying the dissection forward, freeing this fascia radically releases the serratus, allowing all the access of a standard thoracotomy.
The serratus is further dissected off the underlying ribs.
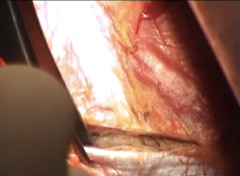
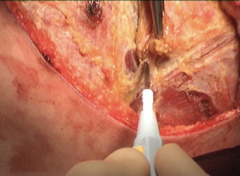
A vertical incision is made along the erector spinae muscles which are then elevated with the cautery to expose the neck of the rib.
The intercostal incision begins well back over the neck of the rib.
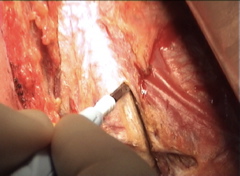
The intercostal incision continues anteriorly, the fibres of the external intercostal muscle directing the blade down away from the neurovascular bundle.
Continuing the intercostal incision well forward allows the same access as a standard thoracotomy, reduces the amount of pressure required to retract the ribs and prevents rib fractures.
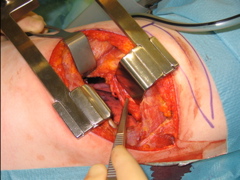
The upper blade of the retractor is now inserted directly adjacent to the rib applying no pressure to the intercostal nerve.
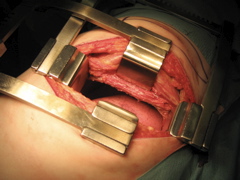
A second De Bakey rib spreader is placed at right angles to the first to retract the latissimus and serratus forward and the trapezius backwards.
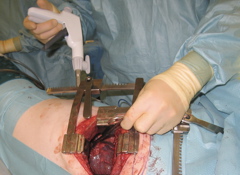
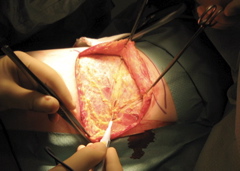
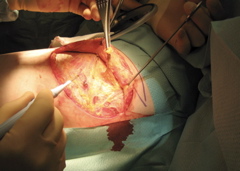
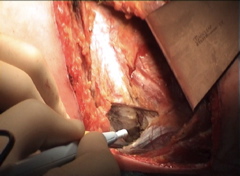
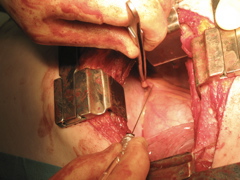
Additional access can be gained by using drain incisions to introduce instruments, as is done in thoracoscopic surgery. In this photo an endoscopic vascular stapler has been placed across the systemic artery feeding an introlobar pulmonary sequestration.
Once the feeding vessel, which arose from the sub-diaphragmatic aorta, had been stapled and divided, the sequestration was wedged out, preserving most of the lower lobe.
Prior to closure, drains are placed and and Chirocaine (long-acting local anaesthetic) is injected into the phrenic nerve fat pad. This reduces shoulder tip pain which often occurs when epidural analgesia is used.
Three or four pericostal sutures are placed to appose the ribs. The sutures are placed in such a way that the neurovascular bundle is elevated. The lower intercostal nerve is protected by the groove in the rib. Drilling holes in the rib or trying to place the suture between the rib and the nerve proved to have no advantage.
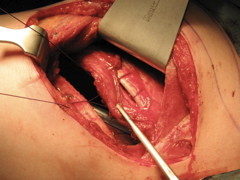
The pericostal sutures are tightened to re-appose the ribs. The intercostal bundle can be seen everted from the wound.

The fascia of the auscultatory triangle is now re-sutured to the latissimus and the trapezius to maintain their anatomical positions.

A Redivac suction drain can be placed to prevent seroma formation.
After placing a stay suture at the midpoint of the fascial layer to ensure the two sides are lined up correctly, the subcutaneous fascia is closed with running Vicryl. To reduce the dead space in which a seroma may form, bites are taken through the deeper tissues with alternate sutures.

A routine subcuticular Vicryl suture closes the skin.

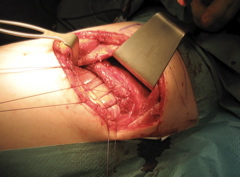
The final result.