Wedge osteotomy (Quicktime movie 22secs 1.0Mb)
Osteotomy sutures (Quicktime movie 28 secs 1.8Mb)

Osteotomy
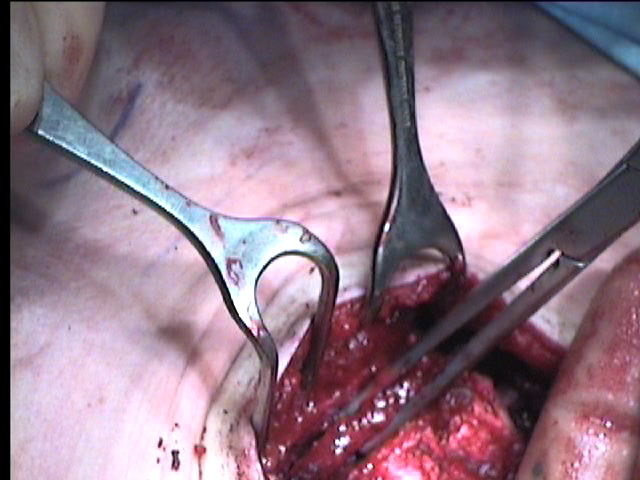
| In the routine excavatum repair the aim is to excise a transverse, anteriorly based wedge of bone from the sternum leaving the posterior periosteum intact. I place the osteotomy between the second and third cartilages to leave the growth centres of the manubrium intact. A generous wedge is then cut using the oscillating saw. The posterior table of the sternum is fractured by bending it backwards increasing the deformity. The wedge can then be removed with forceps. Wedge osteotomy (Quicktime movie 22secs 1.0Mb) |
|
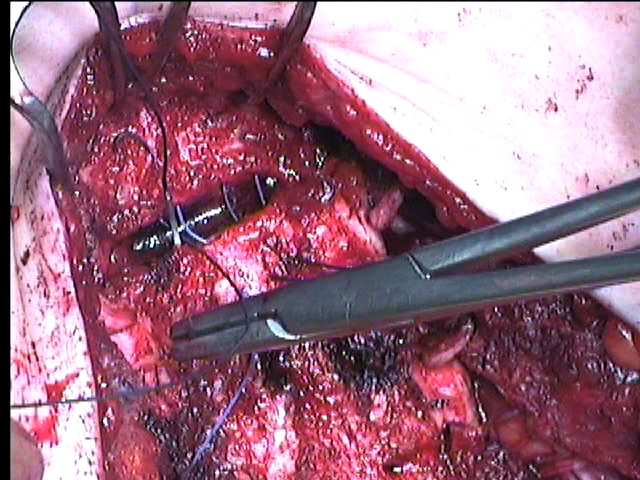
| The deformity is then overcorrected and the heavy Vicryl on a skin cutting needle (Ethicon 9321) used to hold the edges of the osteotomy in place. I use two horizontal mattress sutures, officially holding periosteum but usually through the outer table of the sternum. Osteotomy sutures (Quicktime movie 28 secs 1.8Mb) |
|
| Once tied the sternum should protrude from the incision by itself with absolutely no tension on it. This removes the need for a heavy metal bar to hold it out. | |
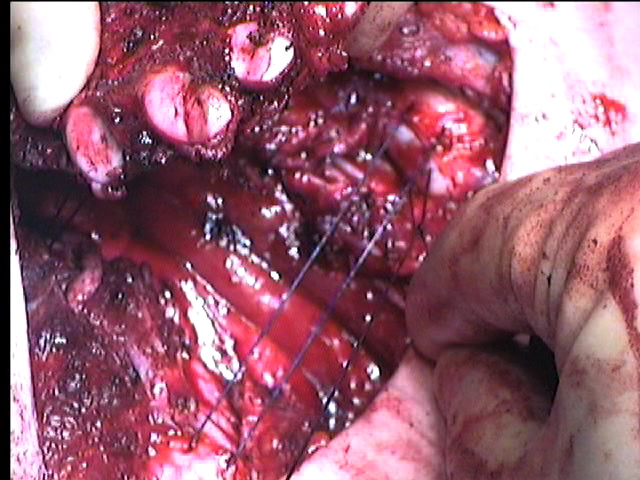
| Two, or in larger children three, mattress sutures are placed deep to the sternum, one at the level of the fourth and another at the sixth costal cartilage, from the tip of one cartilage across to the other. In an excavatum defect I bring the sutures out on the anterior surface of the ribs to gain as much elevation as possible. In a carinatum the reverse holds, with the sutures on the underside of the ribs. PDS supporting suture (Quicktime movie 21 secs 1.5Mb) |
 |
Return to Pectus Index