Thoracic epidural has become the accepted standard for the management of pain in the postoperative period. However, it is a flawed standard and there are times when alternatives need to be considered.
Phrenic nerve block reduces shoulder tip pain.
There are a number of alternatives to epidural analgesia which can be considered when epidural is contra-indicated or where it is not possible to insert an epidural cannula.
-
•For many years we used the patient controlled analgesia (PCA) narcotic system. This can be used either in conjunction with other loco-regional blocks.
-
•Continuous wound infusion with local anaesthetic is also possible and is facilitated by using the commercially available “on-Q Pain Buster” system. This system may be useful for both local infusion and for intercostal or phrenic fat pad infusion.
-
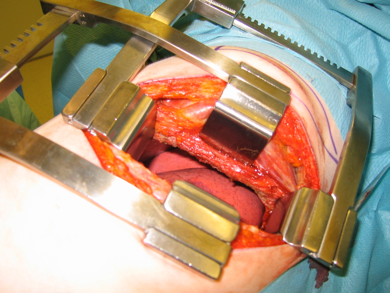
•For open procedures where an epidural is not possible or major VATS procedures we use a continuous intercostal infusion (also known as paravertebral or extra pleural infusion). This is administered using the Pain Buster device.
-
•We use a long acting intercostal nerve block for all other thoracoscopic procedures.
Intercostal neuralgia can be reduced by intraoperative protection of the intercostal nerve and avoidance of pressure imparted by the rib spreader.